
‘More people are going to die’: DoD civilians in Japan face health care access crisis
DoD civilians in Japan say they've lost any meaningful access to on-base healthcare over the last several months, and can't get it from Japanese providers. Defense...
Susan, a primary care psychologist at Marine Corps Air Station Iwakuni, moved to Japan four years ago because she and her husband wanted to experience the world, and a safe country with world-class infrastructure seemed an ideal place to raise their first child.
Now, getting out of the country is a matter of urgency for her family, because of what she and countless other American civilian employees in Japan say have been dire and sudden changes in their ability to access even the most basic health care services.
Susan isn’t her real name. She agreed to speak with Federal News Network only under a pseudonym, afraid that doing so publicly would jeopardize her chances of finding a new job where she can get proper medical care for her daughter, now 10 months old.
“My husband and I chose to go through IVF and bring a child into the world here, because we thought we could properly meet her needs,” she said. “Now I’m living with this guilt — bringing a child into this and not being able to assure her health care. I brought her into a situation where I can’t assure that she’s going to be healthy and fully taken care of.”
The changes that have drastically curtailed health care access for more than 6,000 civilians and an untold number of contractor employees in Japan, though dramatic, vary somewhat from installation-to-installation, and the underlying causes are also multifaceted. Because of that, they’re also difficult to completely resolve overnight.
Defense health officials are quick to point out that there has been no official change in policy: On paper, DoD civilians have always been treated on a space-available or “Space-A” basis at military treatment facilities (MTFs), and active duty service members and their families have the first priority for available appointments. What appears to have changed the most is the department’s definition of what “space available” means.
Seileen Mullen, the acting assistant secretary of Defense for health affairs said the changes civilians are now seeing started when the Defense Health Agency, which recently assumed administrative control of each of the MTFs, determined the facilities weren’t offering enough appointment availability for the active duty and other TRICARE patients it’s required by law to treat as their first priority.
“So what happened, with all good intentions, was we decided we needed to reiterate that policy, which unintentionally squeezed out Space-A spots,” Mullen told a town hall meeting at Kadena Air Base last week. “As we saw more active duty and active duty family members, we had [less Space-A availability]. We could have probably communicated and socialized that better and talked more with people on the ground. But that really didn’t happen.”
DoD civilians living in Japan say although access to health care in the country has always been somewhat challenging, the most recent changes have been dramatic. They happened gradually, and then all at once.
First, in September, some employees started hearing from their regular providers at local MTFs that they’d no longer be able to see them. In some cases, military doctors bade their civilian patients a reluctant adieu by writing prescriptions that extended their medications for as long as possible.
Then, just before Christmas, Maj. Gen. Joseph Heck, DHA’s regional director, issued an updated instruction that explicitly told MTFs that they should only treat Space-A patients for acute, non-recurring health needs.
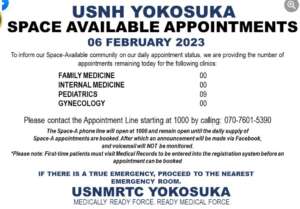
One practical effect of that instruction was that civilians could no longer make medical appointments at MTFs until the day of the visit. If they wanted to be seen, they’d need to check their local facility’s Facebook page at 10am each day to see if the hospital or clinic had any “Space -A” appointments available for the particular category of care they needed, and then try to make an appointment for the same day.
Nicole Casimir, a DoD civilian who works at Yokuta Air Base, said many employees feel as though the rug has been pulled out from under them. Her family’s challenges started in August, when the base’s medical leadership began restricting pediatric care for civilian patients, leaving her son without a reliable source for the ADHD medication and EpiPens he needs for his medical conditions.
“It adds extra stress to a lot of us,” she said in an interview. “I haven’t done much research on how I can continue my own health care because I’m spending so much time trying to get the services that I need for my son. My husband has high blood pressure, so every day I’m worried about if something should happen, he’s not going to be able to get the emergency care that he needs. It’s just everyday stress that’s in the back of your mind while you’re trying to produce for your agency and for the warfighter. We’ve had people at our site that have passed away — one, because that person could not get the emergency care that he needed, and another person because they couldn’t get the mental health treatment that they needed. So it’s real.”
Casimir and other DoD employees say the situation has also already had palpable effects on military commands’ and Defense agencies’ ability to attract and retain employees.
“We have people who want to have the opportunity to work overseas — it’s just such a great experience, not only for being able to see how your agency directly impacts the greater world, but also for our children as well. It just expands them culturally,” she said. “But we’ve had people who will not apply for the positions because they know that there is a health care concern out here, or they apply, delve deeper into the health care situation, and then end up retracting their acceptance. We’ve had other people who just can no longer deal with the stress and uncertainty, and they leave early, so then we have to scramble to backfill their positions.”
But simply leaving Japan isn’t a viable option for some DoD employees.
While some can ask for a transfer to another geographic location within their agency, for others, leaving suddenly is much more financially perilous. One major example is the roughly 2,400 schoolteachers and other employees who work for the DoD Education Activity (DoDEA) in Japan. DoDEA simply does not offer the ability to transfer to another country, numerous employees said.
“The choice that I’m faced with — if I cannot get to an installation or somewhere where I can get health care services — is I have to quit my job,” said one teacher during a town hall last week at the Army’s Camp Zama. “I feel that I provide a good service to this community as a teacher and a head football coach, but I now have to look out for my own kids. I get it, from a resources standpoint, but teachers are left with little to no options. Our options are to either fight it out and maybe find something, or quit.”
Most of the reasons DoD civilians have so few options to “find something” outside of the MTFs have to do with particular nuances involving the Japanese health care system. Employees who’ve served in other areas with large concentrations of American civilian personnel, like Germany and South Korea, say they haven’t encountered similar problems.
But in Japan, DoD civilians have seen varying degrees of difficulty getting appointments at private hospitals and clinics. Some accept American insurance and some do not, but in many cases, they require foreigners to submit up-front payment if they’ll see them at all.
According to Japan Civilian Medical Advocacy, a group of DoD civilians who organized last fall to look for fixes to the health care crisis, Japanese facilities often require payments of up to 200% of their standard fees before they’re willing to treat foreigners. And unlike in the American system, there’s no legal requirement that hospitals or clinics treat anyone, even in emergency situations.
That reality sometimes impacts active duty servicemembers and their families too. Since the military does not operate any of its own trauma centers in Japan, they’re also reliant on Japanese hospitals for higher levels of care.
And cultural differences between the Japanese medical system and the American one also mean that DoD civilians can be denied care at local facilities for reasons they’d never have contemplated.
For instance, one of the most popular childbirth clinics for American women in Okinawa simply will not see patients who’ve been diagnosed with ADHD, said Kelly Pretorius, a pediatric nurse practitioner who has been trying to help women and families in the area find care.
“I have so much respect for the Japanese culture, but the perspective on mental health is drastically different than what we do in America,” she said in an interview. “The approach to pain management is also totally different. You can’t get an epidural in Okinawa — they don’t do that. I don’t know one woman who has been able to get an epidural in Okinawa. And forcing women to have an unmedicated delivery when that’s not their choice is mind-blowing to me. Episiotomies are more common. I have a woman who’s going to have a C-section soon, and her husband’s not even allowed to be in the hospital.”
Pretorius, who is married to a DoD civilian employee, experienced the differences in the Japanese medical system first-hand when she had her own baby at an off-base facility in 2020. After days of labor, she had post-delivery complications that weren’t fully diagnosed until she saw a doctor in the United States, who determined that she now needs major reconstructive surgery.
Despite two masters degrees and a PhD, Pretorius has also been unable to find a job at the Navy-operated MTF in Okinawa, because the hospital had no billets open. The MTF did, however, allow her to work as a pediatric nurse practitioner on a volunteer basis via the Red Cross — something she welcomed, because the unpaid work at least gave her enough clinical hours to maintain her medical license in Texas.
“I was also going out on weekends to do newborn checks for the families, because I just love seeing babies and providing that guidance to new moms, and people have such little support out here that I was happy to offload that patient load to the other practitioners that were working,” she said. “But once this crisis started occurring, I’ve stopped volunteering. Because now all my energy is being spent on this issue.”
During last week’s town hall meetings, senior Defense officials emphasized that they were primarily there to listen to DoD employees’ concerns and learn about the problems before they developed solutions via a working group the department has established to deal with the access to care problem.
Gil Cisneros, the undersecretary of Defense for personnel and readiness, told participants he was surprised to learn that Japanese facilities can turn patients away for any reason.
“The Japanese medical system is not the system that we’re used to, and that’s the big picture right there,” he said. “The whole idea of individuals being turned away when there’s an emergency is just a foreign concept, that you just wouldn’t see in any hospital in the United States. So we’re continuing to grasp the picture here and what everybody’s dealing with. I definitely have a better understanding of how it’s affecting everybody, a lot clearer than I did before I got here.”
And aside from DHA’s lack of communication with DoD civilians about the sudden changes in its interpretation of “space available” at MTFs, Cisneros said it also appeared that DoD components hadn’t adequately informed job candidates about the military’s Space-A policy, what it would mean if it were fully enforced, and the realities of the Japanese health care system.
Indeed, in interviews and town hall testimonials, numerous employees said they’d been told they would receive all of their health care via MTFs when they agreed to take positions in Japan.
“I have had my prescriptions written for me by the base hospitals for the past 13 years for my chronic condition. I have one more refill. What am I supposed to do? I’m currently making poor choices to extend my medication for as long as I can, because I’m almost 100% certain I’m not going to be able to get my medications refilled,” one employee said at the Camp Zama session.
As of Monday, the Defense Department had not responded to questions about how soon the civilian medical task force would arrive at its recommendations, or whether Cisneros would order any immediate changes to care in Japan prior to the completion of the task force’s work.
In a statement, Peter Graves, a spokesman for the Defense Health Agency, said DHA understands the importance of access to care for DoD civilians.
“Our mission set includes installation support in Japan that directly translates into providing as much space available appointments as we can to non-beneficiaries who support their installation as well as their tenant commands. To do this for both our enrolled population and also those civilians who support the installation, we need to optimize the ability of our clinics and hospitals to see more patients, which we are doing and will continue to do across the military medical treatment facilities in Japan,” he said. “But it is also our responsibility to effectively communicate when we cannot provide care either due to a lack of capability where we do not have the ability to provide that specific service to anyone, or if we have a lack of capability, and therefore we are limited in the number of patients we can provide our services. The bottom line is we will always do what we can to take care of the patient. Always.”
Japan Civilian Medical Advocacy has suggested several specific actions the department could take to resolve the crisis.
Some are difficult and long-term, like sizing the mission of each MTF to fully account for the medical needs of the DoD civilian population, rather than the current practice of resourcing the clinics and hospitals solely based on the number of active duty service members in a particular facility’s area of responsibility. Others, in theory, could be done more quickly, like letting civilians get prescriptions written by state-side providers, but filled at MTF pharmacies.
Heck said that’s one of the short-term options DHA is exploring.
“We’re working on a solution to the prescribing issue so that prescriptions can be sent from a U.S.-based provider to the MTF here, with the exception of any narcotic drugs,” he said. “And as far as telehealth is concerned, we are looking at ways that we may be able to offer telehealth from the states to a location that’s somewhere on a U.S. installation. So you wouldn’t be able to do the telehealth appointment from your home, but if you’re on base, we may be able to get around the licensing issues. We’re exploring that as well.”
But employees stress the proper time for exploration of these issues was many months ago, before DoD implemented the restrictions on MTF care for civilians.
Now that it’s a crisis, the department needs to act accordingly, they argue.
“I am genuinely concerned that more people are going to die unless this policy is revoked immediately,” Pretorius said during a town hall at Kadena Air Base. “Why aren’t you rescinding this policy until there’s a solution that your working groups have achieved? And now that you understand the situation, would you move your family here? Can you convince civilians to stay? And why is a stay-at-home mom coordinating the efforts of American citizens desperately seeking medical care, because government agencies have stripped us of our access?”
Copyright © 2025 Federal News Network. All rights reserved. This website is not intended for users located within the European Economic Area.



Jared Serbu
Jared Serbu is deputy editor of Federal News Network and reports on the Defense Department’s contracting, legislative, workforce and IT issues.
Follow @jserbuWFED
Related Stories

Moving more TRICARE patients to civilian care would cause ‘significant harm,’ study finds

